Exam Description
- 2.5 hour “open book” examination
- 100 multiple choice questions
- At Exam Check-in time, candidates must present 2 forms of Identification, one of which must be a valid government-issued ID.
- Content based on the current HOPE data collection rules and guidance provided by CMS (Visit our products page).
- Exam results are reported as Pass or Fail.
- Exam score is based on the number of questions answered correctly. Unanswered questions will be considered as answered incorrectly.
General Guidance
- Arrive at least 30 minutes prior the exam time to sign-in and get settled.
- Candidates should be signed in and seated 15 minutes before exam start time. Late arrival may reduce available testing time for the late candidate; no extra time will be provided.
- Exam is open book & open notes: Candidates are allowed to bring ANY paper-based HOPE reference materials into the examination, including, HOPE Guidance Manual, CMS HOPE FAQs, the HOPE in Action handout materials, and an INSTANT HOPE Answers book. Reference materials may include handwritten notes, loose notes, tabs and flags as page markers.
- Electronic equipment of any kind may not be used in or out of the exam room during the testing time. Cell phones will be turned off.
- At a Paper & Pencil test, beverages are permitted in the testing environment at your own risk. No additional time is given to clean up a spill. At Computer-Based Tests (CBT), no beverages are allowed in the testing room.
- Food is not allowed in the exam room except for medical reasons.
- Independent study of the current HOPE data collection rules and guidance provided by CMS is encouraged though is not required.
- Successful candidates will understand the HOPE assessment timepoints, will understand intent of each HOPE item, and will have a working familiarity with all the HOPE conventions and special circumstance instructions included in the HOPE Guidance Manual and related CMS FAQs. Candidates may be presented with a question that is testing knowledge of a fact regarding a HOPE item. Alternatively, candidates may be presented with a scenario, and asked to determine which response option should be selected for a particular HOPE item, based on the details provided in the Exam scenario. The Exam scenario will provide all the details needed to successfully apply the CMS guidance and select the single correct response. The Exam is open book, so as time allows, candidates will be able to consult their references as needed.
- Use the domain descriptions below as a guide for any exam review and preparation and try the sample questions that are included.
Description of CHS-C Exam Domains with Sample Questions and Study Resources
- Time Points & Symptom Follow-up Visits Domain
- Patient Populations Domain
- HOPE Regulations Domain
- Section A – Administrative Information Domain
- Section F – Preferences Domain
- Section I – Active Diagnoses Domain
- Section J – Health Conditions Domain
- Section M – Skin Conditions Domain
- Section N – Medications Domain
- Section Z – Record Administration Domain
This Domain tests on your knowledge of situations and events which trigger a mandatory HOPE assessment. You will need to understand when HOPE data for Admission and Discharge is required to be collected. You will also need to be able to identify when HOPE Update Visits (HUV1, HUV2) are required. A clear understanding of the conditions and timing of conducting required Symptom Follow-up Visits (SFVs) will also be necessary. You could be presented with questions requiring you to understand the definitions and circumstances when HOPE assessments or SFVs are required, as well as being able to apply relevant guidance to providing accurate HOPE coding based on offered patient scenarios.
Sample Question for this Domain:
Question: Which of the following statements is true regarding the Symptom Follow-Up Visit (SFV)?
- An SFV must be completed after every HOPE timepoint
- The SFV must be a separate visit from the Admission or HUV
- The SFV cannot occur on the same day as the admission
- An SFV can only be conducted by an RN
Correct Response (B)
This Domain tests your knowledge of CMS HOPE guidance related to which patients HOPE data collection applies to. You may be presented with scenarios that include information such as the patient’s age, payer, discharging facility, admitting or changing site of service, or events occurring during the patient’s hospice care to determine if HOPE data collection would be required.
Question: Which of the following patients is excluded from completion of HOPE?
- Patients who expire during the hospice admission visit
- Patients receiving more than 1 hospice visit, but who have a length of stay of less than 3 days
- Patients who elect the hospice benefit but who expire prior to the admission visit
- Patients who refuse to respond to the HOPE assessment items
Correct Response (C)
This Domain tests your knowledge of the CMS HOPE Regulations regarding HOPE data collection. Specifically, you will need to have a good working knowledge of how the HOPE data collection requirements align with the Hospice Conditions of Participation (CoPs) related to the comprehensive assessment at admission and at update timepoints. You will also need to have an understanding of the criteria required to determine that a patient should be considered “admitted” to hospice, for the purposes of requiring HOPE.
Question: A patient is admitted to hospice on 11/25/20XX and consents were signed on the same day. After the admission visit, the patient reconsidered, deciding they wanted to continue curative treatment and revoked their hospice election. Which HOPE timepoints are required to be collected and submitted?
- HOPE Admission record only
- Both the HOPE Admission and Discharge records
- HOPE Discharge record only
- No HOPE records need to be collected
Correct Response (B)
This Domain tests your knowledge of the CMS HOPE guidance related to coding items that collect information on patient characteristics and demographics.
Question: During the admission visit, a patient’s spouse informs the nurse that the patient has traditional Medicare for their hospice care as well as private insurance that is available to them for prescriptions and DME. They also have some private funds set aside for co-pays. What is the best response for A1400 – Payer Information?
- A. Medicare (traditional fee-for service)
H. Private Insurance/Medigap
J. Self-Pay - A. Medicare (traditional fee-for service)
B. Private Insurance/Medigap - A. Medicare (traditional fee-for service)
J. Self-Pay - A. Medicare (traditional fee-for service)
Correct Response (A)
This Domain tests your knowledge of the CMS HOPE guidance related to coding the preference items related to evidence of discussions related to the hospice patient’s preferences regarding life-sustaining treatments and spiritual care.
Question: You are admitting a patient onto hospice services on 11/15/20XX. When reviewing the clinical record, you note that the patient has a POLST form that was completed in the prior care setting. The POLST indicates the desire to avoid hospitalization and is dated 11/01/20XX. The POLST is incorporated into the medical record, stating the patient’s preference related to hospitalization. No additional discussion or documentation regarding the topic occurs. What is the best response for F2200A – Was the patient/responsible party asked about preference regarding hospitalization? And F2200B – Date the patient/responsible party was first asked about preference regarding hospitalization be coded?
- F2200A – 1 – Yes, and discussion occurred
F2200B – 11/15/20XX - F2200A – 0 – No
F2200B – skipped - F2200A – 1 – Yes, and discussion occurred
F2200B – 11/01/20XX - F2200A – 0 – No
F2200B – 11/15/20XX
Correct Response (B)
This Domain tests on your knowledge related to coding the Principal Diagnosis and Comorbidities and Co-existing Conditions, following CMS HOPE coding guidance.
Question: A patient is being admitted to hospice with a terminal diagnosis of stage four lung cancer. During the admission she also informs you that she has a history of diabetes and history of breast cancer with resulting mastectomy. Which diagnoses would be coded for I0010 – Principal Diagnosis and which diagnoses would be coded for Comorbidities and Co-existing Conditions?
- I0010 – 01. Cancer
Comorbidities and Co-existing Conditions include I0100. Cancer and I2900. Diabetes Mellitus (DM) - I0010 – 01. Cancer
Comorbidities and Co-existing Conditions include I2900. Diabetes Mellitus (DM) - I0010 – 01. Cancer
Comorbidities and Co-existing Conditions include I0100. Cancer, I2900. Diabetes Mellitus (DM), and I8005. Other Medical Conditions - I0010 – 01. Cancer
Comorbidities and Co-existing Conditions include I0100. Cancer
Correct Response (A)
This Domain tests on your knowledge of CMS HOPE coding guidance related to assessing and documenting physical symptoms and the impact of pain and non-pain symptoms for the hospice patient.
Question: During the HOPE admission visit on 12/17/20XX, your nonverbal patient was observed and determined to have a pain severity rating of moderate on a nonverbal pain scale. The patient’s daughter stated that her mother had been moaning all morning and rarely looked comfortable, constantly clutching their lower abdomen when touched. She also reports that she has been unable to reposition her mother in bed because the patient exhibits signs of distress when someone attempts to move her. The daughter is unsure of any factors that make the pain better. How should J0910 – Comprehensive Pain Assessment be coded?
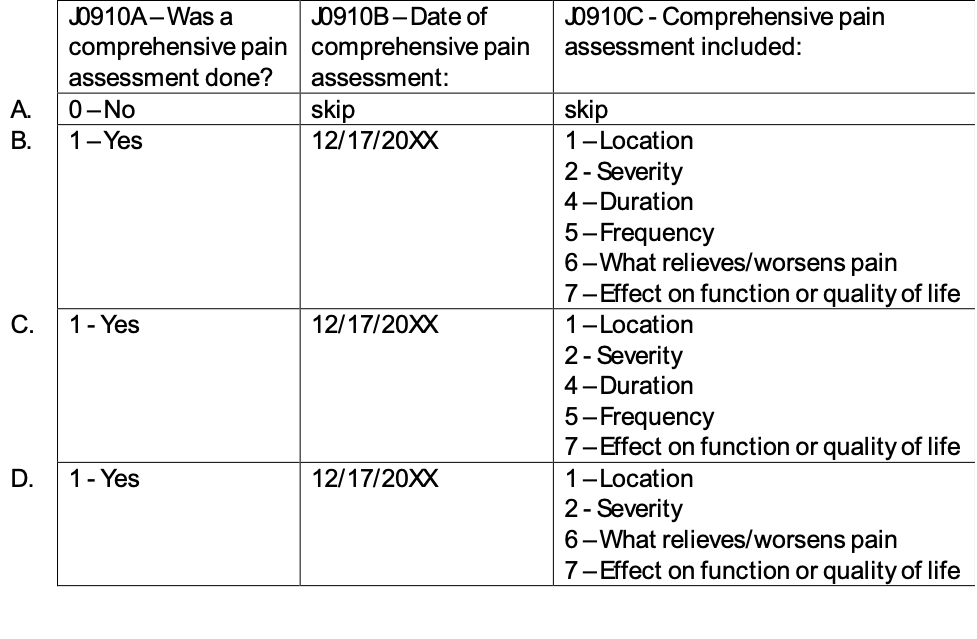
Correct Response (B)
This Domain tests your knowledge of CMS HOPE guidance related to the presence, type and current treatment of various skin conditions that are common in the hospice patient population.
Question: While conducting the HOPE Update Visit (HUV1) a nurse identifies that the patient has a new skin tear on their left arm and a stage 2 pressure ulcer on the left hip. There are no other wounds identified. The patient already has pressure-reducing cushions on their bed and chair, and the nurse educates the patient on frequent repositioning (every 1 ½ to 2 hours) when in bed and when sitting up in a chair to reduce sustained pressure. The nurse also obtains an order for ulcer care with application of a dressing for the pressure ulcer and treats the skin tear with a nonadherent dressing. What is the best response for coding M1200 – Skin and Ulcer/Injury Treatment?
- A. Pressure reducing device for chair
B. Pressure reducing device for bed
E. Pressure ulcer/injury care
D. Application of nonsurgical dressings – with or without topical medications – other than to feet - A. Pressure reducing device for chair
B. Pressure reducing device for bed
C. Turning/repositioning program
E. Pressure ulcer/injury care - A. Pressure reducing device for chair
B. Pressure reducing device for bed
C. Turning/repositioning program - A. Pressure reducing device for chair
B. Pressure reducing device for bed
C. Turning/repositioning program
E. Pressure ulcer/injury care
G. Application of nonsurgical dressings – with or without topical medications – other than to feet
Correct Response (D)
This Domain tests on your knowledge of the CMS HOPE guidance related to initiation or continuation of opioid medications and a bowel regimen.
Question: A review of a hospice admission dated 10/25/20XX shows that a patient is not currently taking any prescribed pain medication, but has a comfort kit in the home on stand-by. During the admission visit, the nurse instructed the patient and family on what medications are in the comfort kit including oxycodone for pain, notifying them that further instruction would be provided when any medications in the kit are needed. What is the best response for coding N0510 – PRN Opioid?
- N0510A – 1 – Yes
N0510B – 10/25/20XX - N0510A – 1 – Yes
N0510B – leave blank - N0510A – 0 – No
N0510B – leave blank - N0510A – 0 – No
N0510B – 10/25/20XX
Correct Response (C)
This Domain tests your knowledge on CMS HOPE guidance related to gathering signatures of hospice staff members who contributed to the completion of HOPE items, and of the individual verifying HOPE record completion, and completing the date the assessment was completed.
Question: Which of the following statements is true regarding Section Z – Record Administration?
- For an HUV, the Z0350 – Date Assessment was Completed cannot extend beyond the HUV assessment timeframe
- The single individual who signs Z0400 should be the last clinician who contributed to the HOPE assessment
- One single individual signs Z0500, after verifying that each required item has been completed.
- The person who signs their name in Z0500 is attesting that the assessment is accurate
Correct Response (C)